Answer of Dermatopathology Case 1
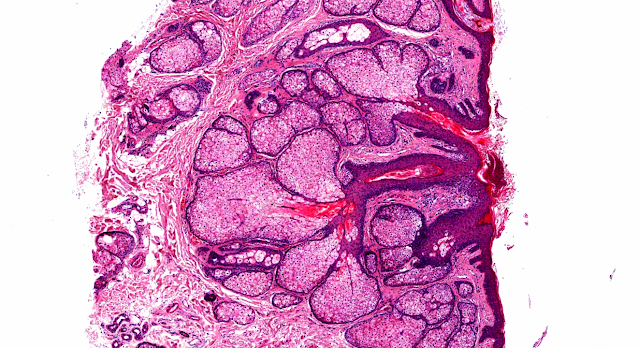
Cutaneous Leiomyosarcoma
Visit: Leiomyosarcoma
Visit: Dermatopathology site
Abstracts:
Cutaneous leiomyosarcoma originating in a symplastic pilar leiomyoma: a rareoccurrence and potential diagnostic pitfall.J Cutan Pathol. 2009 Sep 22.
A case of cutaneous leiomyosarcoma originating in a symplastic pilar leiomyoma isdescribed. The patient was a 60-year-old man who presented with a painless noduleon his chest. Thorough clinical examination did not reveal any evidence of tumor elsewhere. A punch biopsy was performed which showed a benign spindle cellneoplasm with focal cellular pleomorphism that had smooth muscle differentiation and was clearly originating from the arrector pili muscle, consistent with acutaneous symplastic pilar leiomyoma. Immunohistochemical studies were performed and the tumor cells were strongly positive for smooth muscle actin (SMA) anddesmin. Given the clinical information of a mass on the chest, clinicalevaluation was recommended and a re-excision was performed. Histologically, there-excision showed two distinct populations of cells. The upper portion of thetumor mirrored the initial biopsy; however, the base of the tumor showed hypercellular areas composed of spindle cells with marked pleomorphism andincreased number of mitoses. The diagnosis of a cutaneous leiomyosarcomaoriginating in a symplastic pilar leiomyoma was given. This is the first reportof this association of such occurrence reported in the literature. Fons ME,Bachhuber T, Plaza JA. Cutaneous leiomyosarcoma originating in a symplastic pilarleiomyoma: a rare occurrence and potential diagnostic pitfall.
Cluster analysis of immunohistochemical markers in leiomyosarcoma delineatesspecific anatomic and gender subgroups. Cancer. 2009 Sep 15;115(18):4186-95.
BACKGROUND: Leiomyosarcoma (LMS) can be categorized into uterine, retroperitoneal, non retroperitoneal soft tissue, cutaneous, visceral, and osseousanatomic subtypes. The differential expression of smooth muscle markers, estrogenreceptor (ER), progesterone receptor (PR), and Wilms tumor-1 protein (WT1) by anatomic subtype and gender was explored. METHODS: A total of 78 LMS comprised of30 uterine and 48 nonuterine tumors were studied. Nonuterine tumors were comprised of 17 soft tissue, 16 retroperitoneal, 7 cutaneous, 5 visceral, and 3 osseous subtypes. Immunohistochemical staining intensity on tissue microarrayslides was scored as 0, 1+, or 2+, and cluster analysis was performed on the data. RESULTS: Smooth muscle actin was the most sensitive antibody (95%),followed by muscle-specific actin (91%), calponin (88%), desmin (73%), caldesmon (66%), and myosin (64%). Caldesmon and myosin were usually coexpressed, and were highest in retroperitoneal tumors (94%). There was no discernable correlationnoted between histologic differentiation and smooth muscle marker expression. ER was much more common in women, with the highest frequencies noted in female retroperitoneal (86%) and uterine (63%) tumors. Nuclear WT1 was expressed in 11% of all tumors, and was limited to ER-positive uterine and female retroperitoneal tumors. Cluster analysis segregated 4 groups, most notably 1 driven by ER and PR,with the vast majority being uterine and female retroperitoneal tumors.CONCLUSIONS: Smooth muscle markers demonstrated variable sensitivities in LMS,with a tendency for anatomic subtypes to segregate based on expression patternsof these markers. ER defined a subgroup of uterine and female retroperitonealtumors, and WT1 was limited to such tumors, suggesting a common line ofdifferentiation as well as potential therapeutic targets.

Comments
Post a Comment