Answer of Dermatopathology Case 29
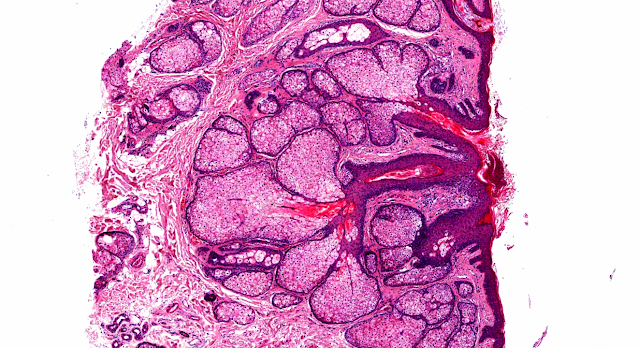
Pilomatrix Carcinoma
Visit: Pathology of Pilomatrix Carcinoma
Visit: Dermatopathology site
Abstract:
Pilomatrix carcinoma presenting as an extra axial mass: clinicopathological features. Diagn Pathol. 2008 Nov 29;3:47.
ABSTRACT: Pilomatrix carcinoma is the rare malignant counterpart of pilomatrixoma, a skin adnexal tumour originating from hair matrix cells. Pilomatrix carcinoma can arise as a solitary lesion de novo, or through transformation of a pilomatrixoma. Pilomatrixoma was first described erroneously as being of sebaceous gland origin but was later discovered to be derived from hair matrix cells. They are rare, slow growing tumours of the skin found in thelower dermis and subcutaneous fat and are predominantly found in the neck and the scalp. While known to be locally aggressive, no malignant form was thought toexist until it was described relatively recently. Since then, approximately ninety cases of pilomatrix carcinoma have been reported.We report the case of a 41 year old mentally retarded male who had a longstanding lesion in the left neck for approximately fifteen years previously diagnosed as a pilomatrixoma. He presented with severe headache, falls and visual disturbance and a biopsy showed pilomatrix carcinoma of the occipital region which, on computed tomography ( CT ) invaded the occipital bone, the cerebellum and the left temporal lobe. At hisinitial presentation he had a craniotomy and subtotal excision of the lesion but received no adjuvant therapy. After an early intracranial recurrence he had further debulking and adjuvant external beam radiotherapy. He has had no further intracranial recurrence after three and a half years of follow-up. Here wepresent the pathological features of this uncommon tumour.
Pilomatrix carcinoma with visceral metastases: case report and review of the literature. J Plast Reconstr Aesthet Surg. 2009 Dec;62(12):e574-7.
Pilomatrix carcinoma, the malignant equivalent of pilomatrixoma, is rare among skin cancers. In the literature, there have been 80 cases of pilomatrix carcinoma reported, and among them nine were with metastases. The clinical presentation of this case is suggestive for the biology and of the usual history of this neoplasm. The patient was a 53-year-old male who had been treated 2 years earlier for a pilomatrix carcinoma located in the posterior part of the neck. The clinical presentation had been characterised by sudden paraplegia caused by vertebral collapse at T4 due to bone metastases. The patient underwent a firstsurgery for vertebral stabilisation and medullary decompression; then, he had a second operation for the resection of the local relapse of the tumour. Literature review and analysis of this case show that the pilomatrix carcinoma should be regarded as a highly locally aggressive tumour, with a high rate of local recurrence as well as metastases.
An unusual composite pilomatrix carcinoma with intralesional
melanocytes: differential diagnosis, immunohistochemical evaluation, and review of the literature. Am J Dermatopathol. 2008 Apr;30(2):174-7.
We report a case of an extremely rare histologic combination of pilomatrix orpilomatrical carcinoma with admixed melanocytes within the same tumor mass. Pilomatrix carcinoma is a neoplasm of low-grade malignancy that is characterized by a tendency for recurrence but low risk of metastasis. A 77-year-old male presented with a nodule on the bridge of the nose that was excised. Histologically, it was typified by asymmetry and poor circumscription, the presence of several variably sized and shaped basaloid aggregations, and surface ulceration. The tumors were composed of pleomorphic basaloid cells with prominent nucleoli and frequent mitoses (some of which were atypical) accompanied by central areas with keratotic material, shadow cells, and foci of necrosis. In addition, intermingled with the pilomatrix carcinoma, several easily identified pigmented cells with dendritic processes were present singly and as smallaggregates. There was no atypia associated with the melanocytic component.Immunohistochemistry revealed the CK14 to be positive mainly within thekeratinizing and the squamous epithelial elements of the tumor. The melanocytic component was strongly immunoreactive for S100, melanoma cocktail (HMB45 andMelan-A), and microphthalmia transcription factor. Pilomatrix carcinoma with melanocytes should be distinguished from the conventional pilomatrixoma with pigmentation, melanocytic matricoma, melanoma, and pigmented basal cell carcinomawith matrical differentiation. Clinicians and pathologists should be aware of the occurrence of pilomatrix carcinoma with melanocytes because of its potential for diagnosis as melanoma. This peculiar lesion recapitulates the intimate relationship existing between matrical epithelium and melanocytes in the embryonal hair follicle or in the anagen stage of the hair cycle. It is possible that sun damage played a role in stimulating migration of melanocytes among matrical cells in this case.

Comments
Post a Comment