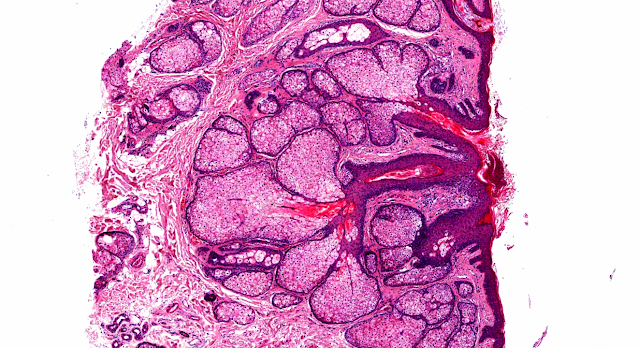
Answer of Dermatopathology Case 31
Reticulohistiocytoma
Visit: Dermatopathology site;
Abstract:
Reticulohistiocytoma (solitary epithelioid histiocytoma): a clinicopathologic and immunohistochemical study of 44 cases. Am J Surg Pathol. 2006 Apr;30(4):521-8.
Reticulohistiocytoma and multicentric reticulohistiocytosis are designations for uncommon, incompletely characterized histiocytic proliferations of the skin or soft tissues. In this study, we analyzed a uniform group of44 lesions composed of epithelioid histiocytes, comprising a subset of lesions originally designated as reticulohistiocytoma, and propose designating them as "solitary epithelioid histiocytoma" (SEH), in line with the recently published classification proposal for histiocytic disorders. There were 26 males and 18 females with a median ageof 35 years (range, 2.5-74 years). All patients had a superficial, circumscribed, mildly elevated, solitary lesion (size range, 1.5-11 mm; median, 4 mm), located in the trunk wall (n = 16), lower extremity (n = 12), head and neck (n = 8,including 2 in the oral cavity), upper extremity (n = 6), penis (n = 1), and an unspecified site (n = 1). Histologically, the lesions typically involved upperand mid-dermis and were not ulcerated. They were composed of large epithelioid histiocytes with a varying number of lymphocytes and neutrophils. The histiocytes had abundant, typically densely eosinophilic, cytoplasm and mostly mild, if any, nuclear atypia. Multinucleated forms with randomly oriented nuclei were alsopresent. The histiocytes had low mitotic activity (range, 0-4 mitoses per 10 wide HPFs; median, 1 mitosis per 10 HPFs). The lesions contained varying numbers of CD3-positive T cells, whereas B lymphocytes, plasma cells, eosinophils, and mast cells were scant, if present at all. Immunohistochemically, the epithelioidhistiocytes were positive for CD163, CD68, lysozyme (variably), and vimentin.They often had focal nuclear immunoreactivity for microphthalmia transcription factor, and they sometimes had focal reactivity for Factor XIIIa and S-100protein. Membrane positivity for CD31, CD43, and CD45 was variable. The epithelioid histiocytes were consistently negative for CD3, CD20, CD30, HMB45,and keratins. All 12 patients with follow-up information had an uneventful clinical course with no recurrences (median, 13 years). SEH is a benign, probablyreactive, histiocytic proliferation of unknown etiology. It needs to be distinguished from Rosai-Dorfman disease, juvenile xanthogranuloma, a variety of granulomatous conditions, and some malignant neoplasms, including histiocyticsarcoma, melanoma, and epithelioid sarcoma.
Reticulohistiocytoma involving the skin, subcutaneous tissue and a regional lymph node.Pathol Int.1996 Jul;46(7):531-7.
A 30-year-old female complained of a surface-eroded solitary nodule on the right thigh.
Histologically, the dermal lesion consisted of uniform-sized polygonal cells with eosinophilic, 'ground glass' cytoplasm. Mitoses were infrequent. Under the histopathologic diagnosis of amelanotic melanoma, wide resection of the skin and dissection of the inguinal lymph nodes were performed. The subcutaneous tissue and a lymph node showed nodular proliferation of histiocytoid cells, in association with hemosiderin-laden multinucleated giant cells. The mononuclear cells were immunoreactive for factor XIIIa, while the multinucleated cells were positive for CD68, lysozyme and HLA-DR. In the lymph node tissue, a considerable number of mononuclear cells positive for CD68 were noted. CD34, alpha-smooth muscle actin, desmin and HMB45 were negative. Ultrastructurally, the mononuclear cells were rich in 100 nm vesicles and 180-350 nm lysosome-like granules. Interdigitation of the plasma membranes was seen in the multinucleated cells. The patient did not complain of joint symptoms, and has been disease-free for 5 years. The histologic and immunohistochemical features are consistent with so-called 'reticulohistiocytoma', though the site of histiocytic growth was unusual.
Reticulohistiocytoma and multicentric reticulohistiocytosis. Histopathologic and immunophenotypic distinct entities. Am J Dermatopathol. 1994 Dec;16(6):577-84. Am J Dermatopathol. 1995 Dec;17(6):625-6.
The clinicopathological and immunohistochemical features of four patients with systemic multicentric reticulohistiocytosis (MR) were compared with five cases of solitary and one case of multiple reticulohistiocytoma (RH), which were confined to the skin only. The MR cases mostly affected the limbs of older women, while RH affected young male adults without preference to site. Characteristically, both entities consisted of oncocytic mononuclear histiocytes (with granular eosinophilic cytoplasm similar to oncocytic thyroid cells) and multinucleated histiocytes with a ground-glass appearance, which appeared to be much larger (> 200 microns) and bizarre in cases of RH compared with cases of MR (50-100 microns). In RH a variable number of vacuolated, spindle-shaped, and xanthomatized mononuclear histiocytes were also present. Immunohistochemical profiles showed positivity of mononuclear histiocytes with HHF35, factor XIIIa, and LN3 (HLA-DR), with a variable number of multinucleated histiocytes in RH showing binding with peanut agglutinin. In mono- and multinucleated histiocytes in both entities macrophage markers KP1 (CD68), KiM1P, HAM56, lysozyme, and alpha 1-antitrypsin were positive. However, macrophage markers MAC387 (L1 antigen) and Leu-M1 (CD15) were negative. Vimentin was universally positive in both conditions, with all other markers (S100, desmin, smooth muscle-specific actin, and QBEnd 10 [CD34]) negative. This study shows that histology supplemented by immunocytochemistry delineates MR from RH and immunohistochemical profiles indicate a cell lineage relationship between RH and adult xanthogranuloma.
Solitary reticulohistiocytoma in pregnancy: immunohistochemical and ultrastructural study of a case with unusual immunophenotype.J Cutan Pathol. 1995 Apr;22(2):177-81.
A case of a solitary reticulohistiocytoma during pregnancy is reported. The tumor arose on the right thigh of a 31-year-old woman during the 2nd month of gestation. Physical examination 6 months later revealed a 9 x 6 mm yellowish white papule. A biopsy showed a dermal proliferation of spindle to polygonal cells embedded in fibrous tissue with admixed neutrophils, eosinophils, and lymphocytes. Immunohistochemistry was positive for S-100, factor XIIIa, HLA-DR, KP-1, vimentin, and neuron-specific enolase. Ultrastructurally, the cells showed abundant lipid, lysozomes, and endoplasmic reticulum. No Birbeck granules could be identified. The results suggest an aberrant immunophenotype intermediate between indeterminate cells and dermal dendritic cells. The relationship of these lineages to reticulohistiocytoma and other dermal proliferative disorders is reviewed.
Multicentric reticulohistiocytosis presenting with destructive polyarthritis , laryngopharyngeal dysfunction, and a huge reticulohistiocytoma. J Clin Rheumatol.2006 Oct;12(5):252-4.
Multicentric reticulohistiocytosis (MRH) is a rare multisystemic disease presenting with skin lesions and erosive polyarthritis and is often associated with malignancy. We describe a 60-year-old woman with diffuse papulonodular skin eruptions and progressive osteolytic bone damage over the bilateral hands, humeral head, and acromioclavicular joints within 2 years. Moreover, dysphagia and a hoarse voice occurred in this patient and an unusual huge mass reticulohistiocytoma--developed over the left upper back. Tissue biopsy of the skin lesions, laryngeal nodules, and this large mass showed infiltration of numerous CD68(+) histiocytes and multinucleated giant cells with abundant eosinophilic ground-glass cytoplasm. Combination therapy with steroids and methotrexate improved her cutaneous, joint, and laryngopharyngeal symptoms. The large reticulohistiocytoma resolved with methylprednisolone pulse therapy. This polyarthritis, which can be confused with rheumatoid arthritis, can be diagnosed by careful immunohistochemical examination of biopsies. To prevent the irreversible disease process, early and aggressive therapy is necessary.

Comments
Post a Comment