Answer of Dermatopathology Case 42
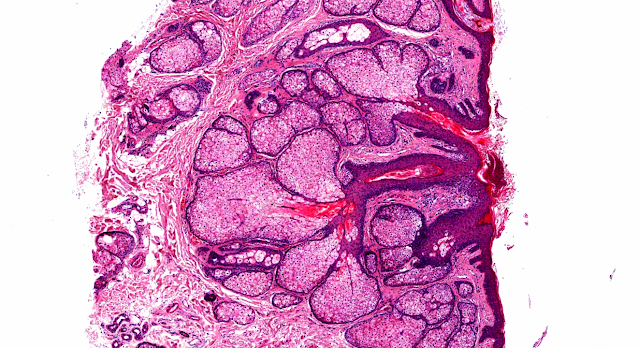
Lupus Panniculitis (Lupus Profundus)
Visit: Dermatopathology site
Abstract:
Normal subcutaneous fat, necrosis of adipocytes and classification of the panniculitides.Semin Cutan Med Surg.2007 Jun;26(2):66-70.
The panniculitides represent a group of heterogeneous inflammatory diseases that involve the subcutaneous fat. The specific diagnosis of these diseases requires histopathologic study because different panniculitides usually show the same clinical appearance, which consists of erythematous nodules on the lower extremities. However, the histopathologic study of panniculitis is difficult because of an inadequate clinicopathologic correlation and the changing evolutive nature of the lesions. In addition, large scalpel incisional biopsies are required. From histopathologic point of view, all panniculitides are somewhat mixed because the inflammatory infiltrate involves both the septa and lobules. However, nearly always the differential diagnosis between a mostly septal and a mostly lobular panniculitis is straightforward at scanning magnification on the basis of the structures more intensely involved by the inflammatory infiltrate. Mostly septal panniculitides with vasculitis are actually more vasculitis than panniculitis and include superficial thrombophlebitis and cutaneous polyarteritis nodosa. Mostly septal panniculitides with no vasculitis include erythema nodosum, necrobiosis lipoidica, deep morphea, subcutaneous granuloma annulare, rheumatoid nodule, and necrobiotic xanthogranuloma. Mostly lobular panniculitis with vasculitis is only represented by erythema induratum of Bazin. In contrast, mostly lobular panniculitides without vasculitis comprise a large series of disparate disorders, including sclerosing panniculitis, calciphylaxis, sclerema neonatorum, subcutaneous fat necrosis of the newborn, poststeroid panniculitis, lupus erythematosus profundus, pancreatic panniculitis, alpha(1)-antitrypsin deficiency panniculitis, subcutaneous Sweet syndrome, infective panniculitis, factitial panniculitis, lipodystrophy, traumatic panniculitis, subcutaneous sarcoidosis, and sclerosing postirradiation panniculitis. Finally, some cutaneous lymphomas may simulate panniculitis, both from clinical and histopathologic points of view and, for that reason, they will be included in this review, although they are not inflammatory processes, but authentic lymphocytic neoplasms involving subcutaneous tissue.
Lupus erythematosus panniculitis: clinicopathological, immunophenotypic, and molecular studies. Am J Dermatopathol.2010 Feb;32(1):24-30.
Lupus erythematosus panniculitis (LEP) is an inflammatory disorder of the subcutaneous fat in patients with lupus erythematosus (LE). It is a rare variant of the disease, which occurs approximately in 1%-3% of patients with cutaneous LE. The purpose of this study was to investigate the clinical, histopathologic, immunophenotypical, and molecular profiles of LEP. We performed a retrospective study of 19 biopsy specimens from 17 patients with LEP. We reviewed their clinical data and reexamined the histopathology. Immunophenotyping and molecular studies were done using sections from paraffin-embedded formalin-fixed tissue. The most common clinical manifestation was a depressed patch on upper arm. Patients showed good response to variable treatment modalities, but, generally, relapse of panniculitis was noted when treatment was discontinued. Histopathologically, most specimens revealed lymphoplasmacytic lobular panniculitis with epidermal and dermal changes of LE, hyaline fat necrosis, and lymphoid follicles. Immunohistochemistry showed a mixture of T and B cells in dermis and subcutis with a slight preponderance of T cell. Although the polymerase chain reaction analysis of the T-cell receptor-gamma gene rearrangement showed a polyclonal smear in 89.5% of cases, a small portion of specimens demonstrated monoclonality. LEP is a chronic recurrent disease with characteristic features. Its diagnosis is often challenging, and a precise diagnosis is achievable only upon elaborate clinicopathologic correlation and integrated interpretation of all diagnostic criteria.
Lupus profundus, indeterminate lymphocytic lobular panniculitis and subcutaneous T-cell lymphoma: a spectrum of subcuticular T-cell lymphoid dyscrasia.J Cutan Pathol. 2001 May;28(5):235-47.
INTRODUCTION: The diagnosis and classification of lymphocytic lobular panniculitis (LLP) has historically proven to be a difficult challenge. We encountered 32 cases of primary LLP which could be categorized as: 1) lupus erythematosus profundus (LEP) (19 patients); 2) an indeterminate group termed indeterminate lymphocytic lobular panniculitis (ILLP) (6 patients); and 3) subcutaneous T-cell lymphoma (SCTCL) (7 patients). OBJECTIVE: We attempted to better define the subtypes of LLP by morphologic, phenotypic and genotypic features and to correlate those features to clinical presentation and outcome. METHOD: Skin biopsy material was studied by conventional light microscopy, through immunophenotyping performed on sections from paraffin-embedded, formalin-fixed tissue and in some cases on sections of tissue frozen after receipt in physiological (Michel's) medium, and by polymerase chain reaction single-stranded conformational polymorphism analysis to assess for clonality of T-lymphocytes. Clinical features were correlated to histologic, phenotypic, and genotypic analyses. RESULTS: Patients with LEP had a prior diagnosis of LE or overlying skin changes which light microscopically were characteristic of LE. Patients with ILLP had no concurrent or prior history of LE, no systemic symptoms or cytopenias, and a clinical course not suggestive of lymphoma. Cases of SCTCL showed hemophagocytic syndrome and/or lesional progression with demise attributable to the disease. Lesions in all groups showed proximal extremity predilection. Females predominated in the LEP group. The average age of onset was 38, 40 and 55 years in the LEP, ILLP and SCTCL groups, respectively. Cytopenia was seen in 4 LEP patients; 1 also developed fever. In LEP and ILLP, lesions resolved with hydroxychloroquine and/or steroid therapy, with recurrences following cessation of therapy. In the SCTCL group 4 developed hemophagocytic syndrome, 4 died within 2 years of diagnosis, and 3 went into remission following chemotherapy. The LEP and SCTCL groups manifested histological similarities: dense perieccrine and lobular lymphocytic infiltration, lymphoid atypia, histiocytes with ingested debris, eosinophilic necrosis of the fat lobule and thrombosis. The atypical lymphocytes although pleomorphic did not have a cerebriform morphology. The infiltrate in ILLP had a similar cytomorphology and distribution with variable angioinvasion which in all save one case was of lesser intensity and was not associated with significant fat necrosis or vasculitis. Germinal centers, dermal/subcuticular mucin deposition and an atrophying interface dermatitis with hyperkeratosis and follicular plugging were largely confined to the LEP group. Erythrophagocytosis, characteristic of SCTCL, usually indicated a supervening subcuticular lymphoid dyscrasia when encountered in ILLP and LEP. SCTCL showed a selective loss of CD5 expression with or without diminution in CD7 and monoclonal CD3 expression. Of 4 cases studied, 3 showed a CD8 dominant infiltrate while 2 others exhibited CD56 and CD30 positivity, respectively. All cases of SCTCL with amplifiable DNA showed T-cell clonality. Similar molecular and phenotypic features indicative of subcuticular lymphoid dyscrasia were encountered in cases of LEP and ILLP including a reduction in CD5, CD7, and/or monoclonal CD3 expression, a preponderance of CD8 lymphocytes within the subcutaneous fat and T-cell clonality. These cases showed lymphoid atypia with variable erythrophagocytosis. Cases of phenotypically abnormal and/or clonal LEP showed one or more of local destruction, lesional size progression, fever, and cytopenias, but lesions responded to hydroxychloroquine and/or prednisone therapy and death attributable to panniculitis could not be documented. Cases that were phenotypically normal and without clonality had none of the aforesaid atypical clinical features. CONCLUSION: Lymphoid atypia, erythrophagocytosis, loss of certain pan T-cell markers, a reduced CD4/8 ratio and TCR rearrangement define subcuticular T-cell lymphoid dyscrasia, including a subset of LEP and ILLP. The subcuticular lymphoid infiltrates represent a spectrum of histologic, immunophenotypic, and molecular abnormalities which range from those which are clearly benign to those which are clearly neoplastic, and also encompasses those cases which defy precise classification into the two aforesaid poles.

Comments
Post a Comment