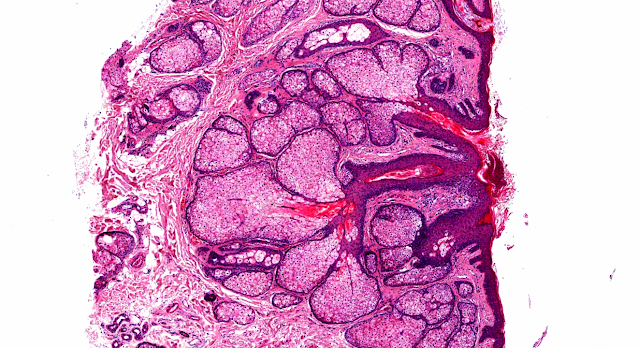
Answer of Dermatopathology Case 57
Erythema Multiforme
Visit: Dermatopathology site
Abstract
Lichenoid histopathologic changes in patients with clinical diagnoses of exfoliative dermatitis. Am J Dermatopathol.1991 Aug;13(4):358-64.
Among 30 patients who received a clinical diagnosis of exfoliative dermatitis and were biopsied between 1982 and 1990, nine showed microscopic features of lichenoid dermatitis. Clinical information was available in eight of these cases. Possible etiologic factors included lymphoma, herpes simplex infection, connective tissue disease, and (in five cases) reactions to drugs. In each instance, microscopic features included a superficial perivascular lymphocytic infiltrate involving the dermal-epidermal interface, vacuolar alteration of the basilar layer, and individually necrotic keratinocytes at all levels of the epidermis. Such microscopic changes are not usually described in connection with exfoliative dermatitis, with the possible exception of those cases related to lichen planus or lupus erythematosus. Disseminated lichenoid drug eruption is one possible interpretation of the drug-induced cases. Erythema multiforme is another condition that has similar microscopic features and has been associated with drugs (many of which also cause exfoliative dermatitis), infectious agents, neoplasms, and connective tissue diseases. Lichenoid dermatitis can become generalized and clinically mimic and exfoliative dermatitis. Many, but not all, of these eruptions may be triggered by drugs.
[Erythema multiforme. A heterogeneous pathologic phenotype]Minerva Stomatol. 1999 May;48(5):217-26.
The term Erythema Multiforme (EM) include actually a wide range of clinical expressions, from exclusive oral erosions (Oral EM) to mucocutaneous lesions (EM Minor), sometimes with severe involvement of multiple mucosal membrane (EM major, Stevens-Johnson syndrome [SJS]) or with involvement of a large area of the total body surface (toxic epidermal necrolysis [TEN]). However, this terminology is not worldwide accepted and often the various clinical categories show some overlapping features. Among the great number of suspected etiological factors, herpes simplex virus is involved in many cases of EM minor whereas SJS and TEN are caused in 80% of cases by systemic drugs, mainly by anticonvulsivants, sulfonamides, nonsteroidal anti-inflammatory drugs and antibiotics. Several oral EM seem idiopathic, but data on this topic are very few. There is no specific or consistent microscopic and immunopathologic pattern of EM and the diagnosis should be done by excluding other similar diseases. The treatment include the use of antivirals for EM minor, mainly if recurrent, and of immunosuppressants (especially systemic corticosteroids) for SJS. TEN patients require adequate supportive care and often they have to be treated in emergency departments. Finally, patients with exclusive oral lesions may be treated with both topical and systemical corticosteroids.
Correlations between clinical patterns and causes of erythema multiforme majus, Stevens-Johnson syndrome, and toxic epidermal necrolysis: results of an international prospective study.Arch Dermatol.2002 Aug;138(8):1019-24.
BACKGROUND: It was proposed that Stevens-Johnson syndrome and toxic epidermal necrolysis differed from erythema multiforme majus by the pattern and localization of skin lesions.
OBJECTIVE: To evaluate the validity of this clinical separation.
DESIGN: Case-control study.
SETTINGS: Active survey from 1989 to 1995 of 1800 hospital departments in Europe.
PATIENTS: A total of 552 patients and 1720 control subjects.
METHODS: Cases were sorted into 5 groups (erythema multiforme majus, Stevens-Johnson syndrome, Stevens-Johnson syndrome-toxic epidermal necrolysis overlap, toxic epidermal necrolysis, and unclassified erythema multiforme majus or Stevens-Johnson syndrome) by experts blinded as to exposure to drugs and other factors. Etiologic fractions for herpes and drugs obtained from case-control analyses were compared between these groups.
RESULTS: Erythema multiforme majus significantly differed from Stevens-Johnson syndrome, overlap, and toxic epidermal necrolysis by occurrence in younger males, frequent recurrences, less fever, milder mucosal lesions, and lack of association with collagen vascular diseases, human immunodeficiency virus infection, or cancer. Recent or recurrent herpes was the principal risk factor for erythema multiforme majus (etiologic fractions of 29% and 17%, respectively) and had a role in Stevens-Johnson syndrome (etiologic fractions of 6% and 10%) but not in overlap cases or toxic epidermal necrolysis. Drugs had higher etiologic fractions for Stevens-Johnson syndrome, overlap, or toxic epidermal necrolysis (64%-66%) than for erythema multiforme majus (18%). Unclassified cases mostly behaved clinically like erythema multiforme.
CONCLUSIONS: This large prospective study confirmed that erythema multiforme majus differs from Stevens-Johnson syndrome and toxic epidermal necrolysis not only in severity but also in several demographic characteristics and causes.
Analysis of the acute ophthalmic manifestations of the erythema multiforme/Stevens-Johnson syndrome/toxic epidermal necrolysis disease spectrum.Ophthalmology.1995 Nov;102(11):1669-76.
PURPOSE: To evaluate the epidemiology, possible etiologic factors, complications encountered, and treatment administered to a group of patients with ocular involvement in the erythema multiforme/Stevens-Johnson syndrome/toxic epidermal necrolysis disease spectrum who were seen at two large tertiary referral centers over a 34-year period.
METHODS: Hospital records from 1960 to 1994 at the Massachusetts General Hospital and Shriners Hospital for Crippled Children were reviewed for patients with erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis. Only patients fulfilling specific clinical diagnostic criteria and those who received a diagnosis by a dermatologist were included in the review.
RESULTS: A total of 366 patients with erythema multiforme, Stevens-Johnson syndrome, or toxic epidermal necrolysis were identified. Drugs were the most commonly identified etiologic factor in all three conditions: sulfonamides were the most frequently identified agents. Eighty-nine patients (24%) had ocular manifestations at the time of their acute hospital stay. Ocular involvement was seen in 9% of patients with erythema multiforme, in 69% with Stevens-Johnson syndrome, and in 50% with toxic epidermal necrolysis. The ocular problems were more severe in patients with both Stevens-Johnson syndrome and toxic epidermal necrolysis. There was no significant difference between the number of patients who were treated with systemic steroids and those who were not (P = 0.42).
CONCLUSIONS: The erythema multiforme/Stevens-Johnson syndrome/toxic epidermal necrolysis disease spectrum remains an important cause of severe visual loss in a significant number of patients. Systemic steroids used during the acute phase of the disease appear to have no effect on the development of ocular manifestations. Studies on the acute immunopathogenic mechanisms occurring in these disease are warranted if more effective therapies are to be found.

Comments
Post a Comment