Answer of Dermatopathology Case 83
Visit: Dermatopathology site
Asymptomatic nodule on an elderly lady's thumb tip. Hautarzt. 2011 Jan 26.
A 71-year-old woman presented with an asymptomatic growing dermal tumor on her thumb. Clinical picture, ultrasound, laboratory investigations and histology were consistent with the diagnosis of gouty tophus. Pathogenesis, risk factors and therapy of tophaceous gout are discussed.
Gouty tophus of the upper eyelid. Ophthal Plast Reconstr Surg. 2008 Sep-Oct;24(5):404-6.
A 64-year-old man with gout presented with history of an enlarging mass in the left upper eyelid causing mechanical ptosis. The patient underwent excisional biopsy. The histopathologic findings confirmed the diagnosis of gouty tophus of the eyelid.
Role of Melanocortin Receptors in the Regulation of Gouty Inflammation. Curr Rheumatol Rep. 2011 Jan 18.
Gouty arthritis is a form of acute joint inflammation provoked by joint deposition of urate crystals. Although this acute pathology resolves after a few days, the marked degree of inflammation in the joint and-possibly more important to the patient-the excruciating pain it causes require proper therapeutic management. Often deemed a "poor sibling" of chronic joint pathologies such as rheumatoid arthritis and psoriatic arthritis, the increasing incidence of gout makes it a more palatable disease for novel drug discovery programs. This fact, associated with novel insights into the molecular mechanisms activated by the urate crystal deposition, is at the basis of new therapeutics under clinical development for gout, a valid example being the effective targeting of the proinflammatory cytokine interleukin-1. Here we briefly review the current status of antigout drug development and propose another target; our focus is on melanocortin receptor agonists as novel therapeutics for gout and inflammatory arthritides, a prototype of which, the adrenocorticotropic hormone, is already used in clinical settings.
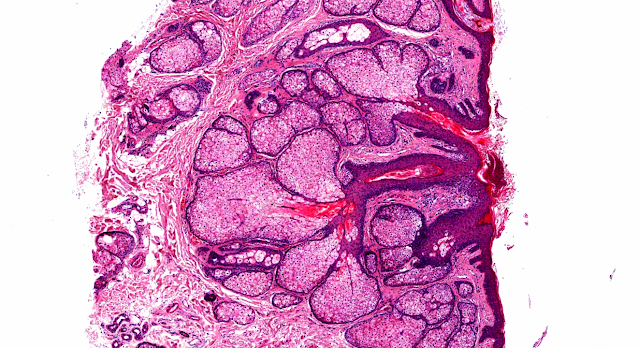
Cellular characterization of the gouty tophus: a quantitative analysis. Arthritis Rheum.2010 May;62(5):1549-56.
OBJECTIVE: To characterize the cellular architecture of the tophus and to determine the presence of cytokines implicated in the initiation and resolution of gouty inflammation.
METHODS: Sixteen fixed, paraffin-embedded, uninfected tophus samples were surgically obtained from 12 patients with microscopically proven gout and were analyzed by quantitative immunohistochemistry. The number of cells present in the corona and fibrovascular zones of the tophus was analyzed by Genmod mixed models analysis.
RESULTS: Numerous CD68+ mononucleated and multinucleated cells were present within the corona zone. Mast cells were identified in all tophus samples and at similar densities throughout the corona and fibrovascular zones. In contrast, neutrophils were rarely observed. Plasma cells were present in very high numbers within the corona zone. The overall number of CD20+ B cells was much lower. However, in 6 of 12 patients (50%), at least 1 B cell aggregate was present in the fibrovascular zone. Large numbers of cells expressing interleukin-1beta (IL-1beta) were observed in the corona zone. Transforming growth factor beta1 (TGFbeta1)-expressing mononucleated cells were also identified. The number of CD68+ cells correlated with the number of cells expressing IL-1beta (r = 0.691, P = 0.009) and the number expressing TGFbeta1 (r = 0.518, P = 0.04).
CONCLUSION: The tophus represents a complex and organized chronic inflammatory tissue response to monosodium urate monohydrate crystals involving both innate and adaptive immune cells. The coexpression of IL-1beta and TGFbeta1 suggests that both proinflammatory and antiinflammatory factors present within the tophus contribute to a cycle of chronic inflammation, attempted resolution, and tissue remodeling.
Large Epidemiologic Studies of Gout: Challenges in Diagnosis and Diagnostic Criteria. Curr Rheumatol Rep.2010 Dec 17.
Large epidemiologic studies of gout can improve insight into the etiology, pathology, impact, and management of the disease. Identification of monosodium urate monohydrate crystals is considered the gold standard for diagnosis, but its application is often not possible in large studies. Therefore, under such circumstances, several proxy approaches are used to classify patients as having gout, including ICD coding in several types of databases or questionnaires that are usually based on the existing classification criteria. However, agreement among these methods is disappointing. Moreover, studies use the terms acute, recurrent, and chronic gout in different ways and without clear definitions. Better definitions of the different manifestations and stages of gout may provide better insight into the natural course and burden of disease and can be the basis for valid approaches to correctly classifying patients within large epidemiologic studies.
Historical review of gout and hyperuricemia investigations. Nippon Rinsho.2008 Apr;66(4):624-35.
Historical development of gout and hyperuricemia investigations was reviewed. Gout has been a recognized disease since the fifth century B.C. In 1683, Sydenham described the detailed clinical features of the disease based on his own condition. Leeuwenhoek (1679) first described crystals in a gouty tophus, which were identified as uric acid by Wollaston (1797). Since uric acid clearance of hyperuricemia was markedly lower than that in normal controls, early investigators considered that the main cause of hyperuricemia was urate underexcretion. However, in the 1940s, studies on uric acid metabolism using isotope tracer techniques demonstrated that a part of hyperuricemia resulted from urate overproduction, which was detected in approximately one-third of all gouty patients. In the 1970s, micropuncture, microinjection and microperfusion methods as well as stop-flow methods demonstrated that uric acid transports in nephron were suspected to consist of four steps, that were glomerular filtration, reabsorption, secretion and postsecretory reabsorption. The majority of filtrated uric acid was almost completely reabsorbed, followed by secretion and postsecretory reabsorption at a proximal site in the tubulus. Each proportion of transports to the glomerular filtration(100%) was estimated approximately 99%, 50% and 40%, respectively. Subsequently, about 10% of the filtrate was excreted in the urine. The authors (1999) suggested that the secretion rate of hyperuricemic patients was significantly lower than that of normal controls but postsecretory reabsorption was not. Therefore, the decrease in the secretion rate was suspected to be the main cause of underexcretion. Dunkan (1960) reported a family demonstrating hyperuricemia associated with severe renal damage that progressed rapidely. Currently, this disease is called familial juvenile hyperuricemic nephropathy (FJHN), and was recently found to be the result of a variation in uromodulin. Enomoto (2002) found a number of urate transporters in the cell surface of the tubulus, among which URAT1 was the most effective in reabsorbing urate from the tubulus lumen to the cells. The urate was released to the blood vessel side by the other transporter OAT. Therefore, URAT1 was suspected to be a cause of underexcretion. As the mechanism underlying overproduction of uric acid, de novo purine nucleotide synthesis has been shown to be increased. In some cases, the increase in de novo synthesis is the result of gene mutation in purine nucleotide synthesis enzymes, such as PRPP synthetase (Sperling, 1973) as well as hypoxanthine guanine phosphoribosylpyrophosphate synthetase (Seegmiller, 1967). However, the mechanism in majority of the overproduction has not yet been clarified and is currently under investigation.

Comments
Post a Comment